

Primary shoulder dislocate peaks in the second and sixth decade
98% of cases, shoulder displaces anteriorly
2% of cases, shoulder displaces posteriorly
95% of first-time shoulder dislocations result from either a forceful collision, falling on an outstretched arm or a sudden wrenching movement
5% of dislocations have an atraumatic origin (minor incidents such as raising the arm or moving during sleep
70% of people who have dislocated can expect to dislocate again within 2 years of the initial injury
Younger and older subjects have a comparable incidence of primary shoulder dislocation
Incidence of recurrent dislocation is much more frequent in adolescent population
Dislocation reported to recur in:
66% to 100% of people aged 20 years or under
13% to 63% of people aged between 20 and 40 years old
0% to 16% of people aged 40 years or older
Anatomy

Image via Complete Anatomy 2018 by 3D4 Medical
Movement Faults

A common movement fault seen in patients that have labral tears is an anteriorly translated humerus. This can be caused from a tight posterior capsule pushing the head of the humerus forward. (Click image to watch 1-2 minute video)
Special Tests

There are many tests to assess if a patient has a labral tear or not. How do you know which one to choose?! Biceps load II has a very high specificity which means that it is an excellent special test for ruling in a labral tear. (Click image to watch 1-2 minute video)
Treatment & Therapeutic Exercise

Treatment depends on stage and irritability of the patient. If the patient has low irritability and primary range of motion impairments have been addressed, it is important to work on movement retraining. This exercise focuses on keeping the head of the humerus centered in the glenoid as the patient work on internal and external rotation. (Click image to watch 1-2 minute video)
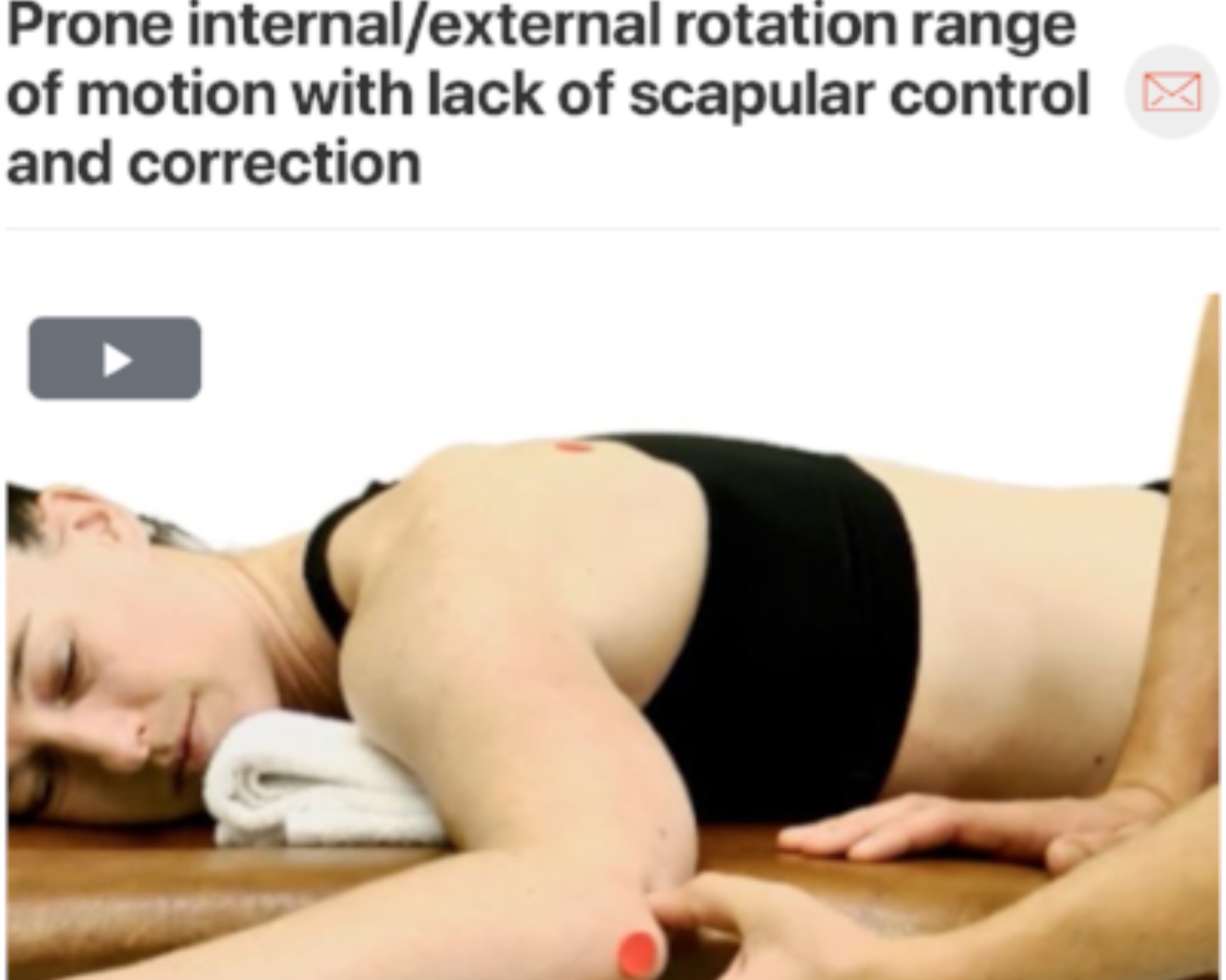
The beauty of movement retraining as a treatment is that it can also be sent home as a home exercise for the patient to work on. The above video shows a progression from working on precision training in supine. Once that is mastered you can progress the patient to prone and then to standing exercises. Quality of motion over quantity is very important to consider with movement retraining! (Click image to watch 1-2 minute video)