From anatomy to discovering the patient!

Cubital tunnel syndrome is the second most common neuropathy involving the upper extremity with an estimated incidence of 24.7 cases per 100,000 person-years.
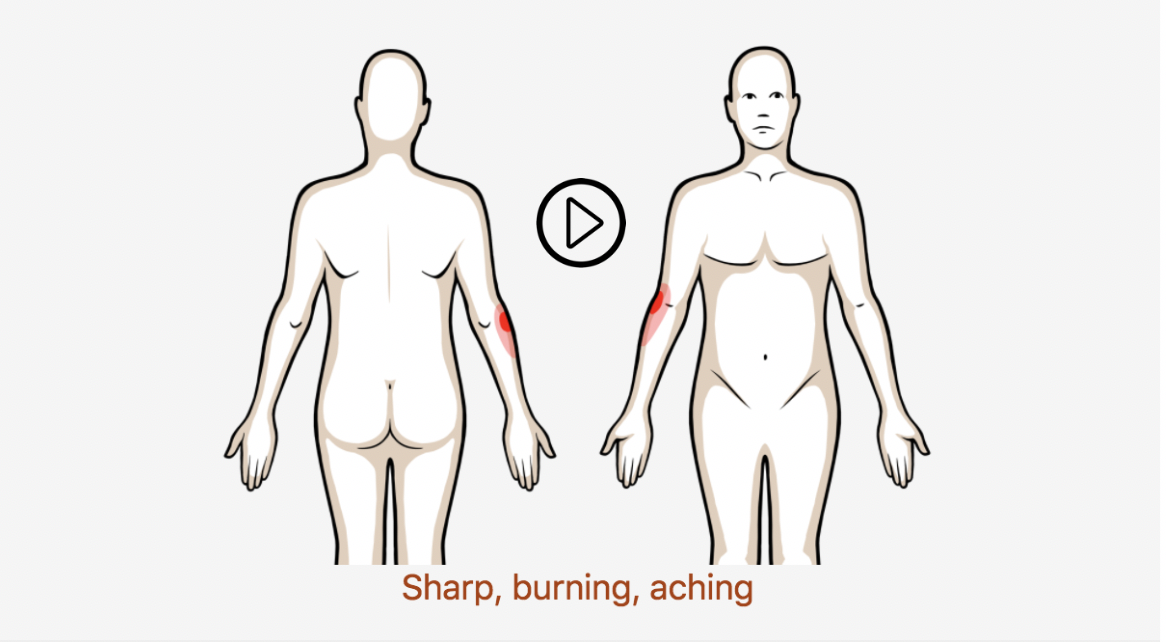
Approximately 40% of people will experience lateral epicondylalgia (LE) at some point in their life
Most common in men and women aged between 35 and 54 years old
Up to 50% of all tennis players also experience some type of elbow pain, with 75 to 80% of these elbow complaints attributable to LE
Approximately 12% of elbow injuries result in contractures requiring surgical release
See more prevalence information in the Clinical Pattern Recognition: Orthopaedics app here
Clinical Pattern Recognition
Click on the pain pattern to learn about the patients and develop your clinical patterns!