

Aside from clinical findings in the subjective exam, patients with adhesive capsulitis will also present with impaired glenohumeral joint range of motion actively and passively (depending on the stage). This restriction typically follows the capsular pattern of the glenohumeral joint: external rotation, abduction, and internal rotation going from most restricted to least restricted. Flexion also tends to be limited and is often accompanied by compensatory shoulder girdle elevation. (Click image to watch 1-2 minute video)
Treatment & Therapeutic Exercise

Treatment depends on stage and irritability of the patient. If the patient has low to moderate irritability and demonstrates capsular restriction, research shows that posterior and inferior glides may be beneficial toward improving pain and range of motion in these individuals! (Click image to watch 1-2 minute video)

Research demonstrates moderate evidence to support the use of stretching exercises in individuals with adhesive capsulitis. Exercises should be matched to patient tolerance; if open chain proves to be too difficult, light closed chain range of motion exercises may be a better choice! (Click image to watch 1-2 minute video)
*Clinical Side Note: When working with individuals with adhesive capsulitis it is important to remember that the process could last 12-18 months with symptoms potentially being present longer. Education on the process and managing patient expectations is an integral part of the rehabilitation process. Depending on the stage of adhesive capsulitis, as well as clinical judgement, it may be beneficial to postpone use of patient visits until progress can be made!
Clinical Pattern Recognition - Neck Pain
From anatomy to discovering the patient!

22% to 70% of the population will have neck pain some time in their lives
At any given time 10% to 20% of the population reports neck problems, with 54% of individuals having experienced neck pain within the last 6 months
Prevalence of neck pain increases with age
Most common in women around the fifth decade of life
See more prevalence information in the Clinical Pattern Recognition: Orthopaedics app here
Meet the 5 common neck pain patients from the Clinical Practice Guidelines!
Clinical Pattern Recognition
Click on the pain pattern to learn about the patients and develop your clinical patterns!
1. Cervical Facet Syndrome/Spondylosis - Neck Pain and Mobility Deficit (1-minute video)

2. Cervical Radiculopathy - Neck Pain and Radiating Arm Pain (1-minute video)
3. Whiplash - Neck Pain and Movement Coordination Impairments (1-minute video)

4. Neck sprain/strain - Neck Pain and Movement Coordination Impairments (1-minute video)

5. Cervicogenic headache - Neck pain and headache (1-minute video)

Cervical Facet Syndrome/Spondylosis
Neck Pain with Mobility Deficits

Patients with cervical facet syndrome or spondylosis tend to present with unilateral neck pain and complaints of limited range of motion. Pain can also be referred to the scapula and shoulder regions! If you do not know the common clinical findings no problem! Click here
Anatomy
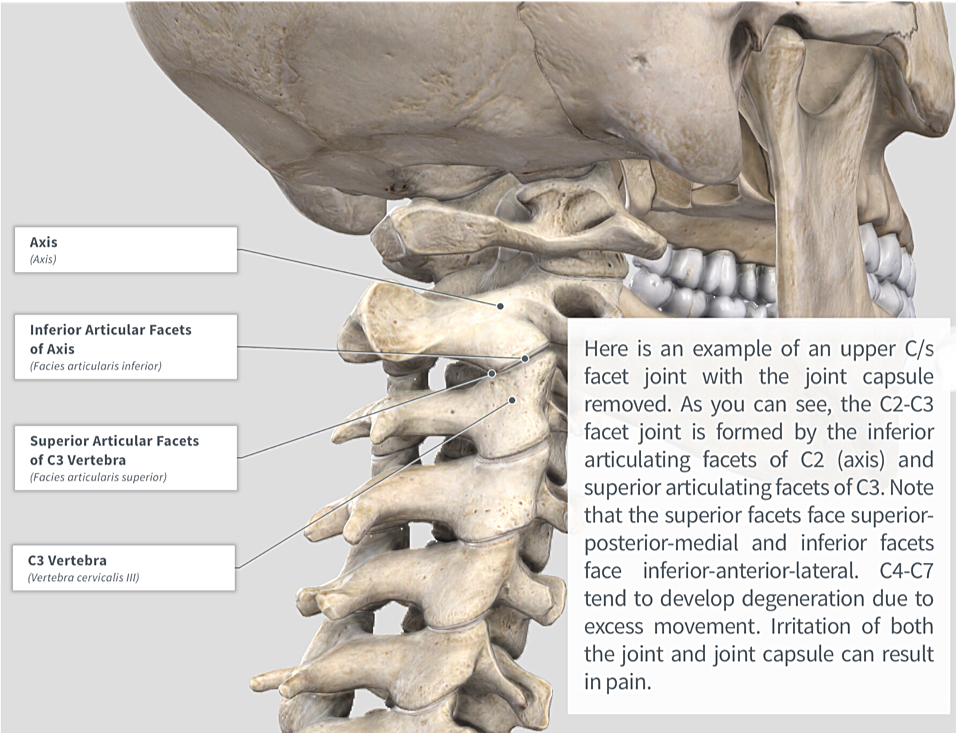
Image via Complete Anatomy 2018 by 3D4 Medical
Key Finding

The cervical spine quadrant assessment elicits maximal strain to the facet joints via coupling of side bend, rotation and extension movements. Although discomfort is common with this test, if the patient experiences reproduction of their primary complaint the likelihood of facet pathology is increased. (Click image to watch 1-2 minute video)
Treatment

If the patient meets the criteria and is deemed appropriate, the patient may benefit from cervical spine thrust manipulation! Research shows that thrust manipulation and/or non-thrust mobilization in conjunction with therapeutic exercise produces better outcomes than either treatment alone! (Click image to watch 1-2 minute video)
Therapeutic Exercise

After improving range of motion it is important to instruct the patient on how to move properly in this new range! (Click image to watch 1-2 minute video)
*As always, remember to assess the whole individual and do not forget to address other impairments, which may be contributing to the patient’s primary complaint!
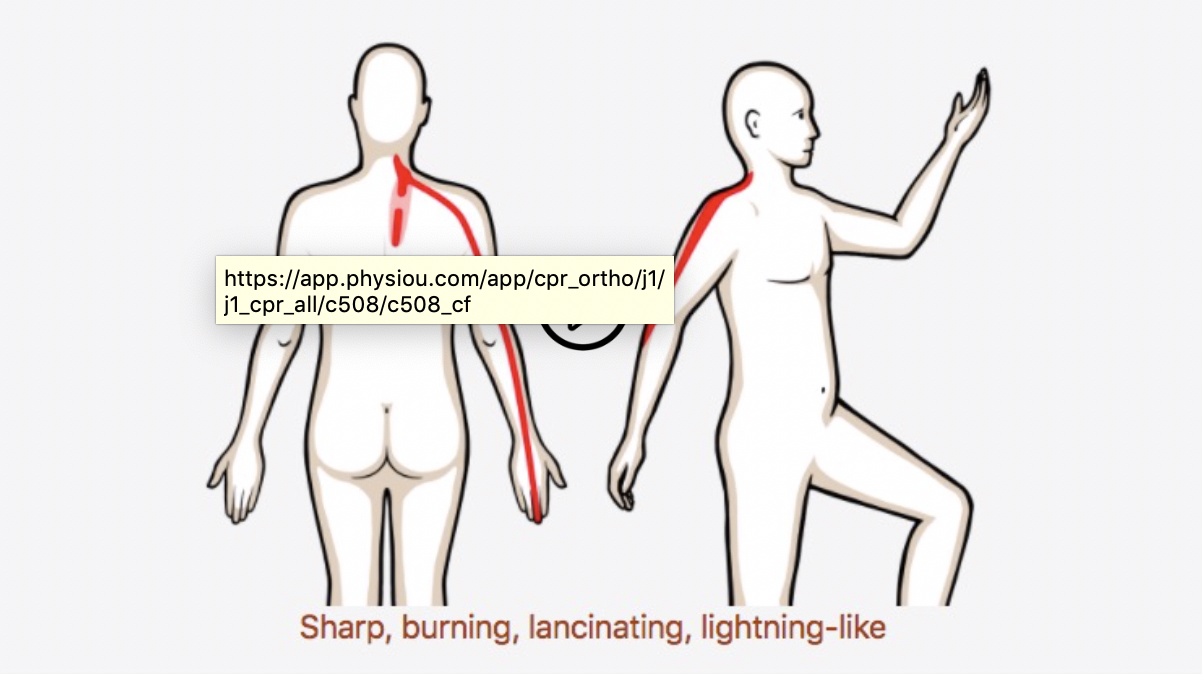
Cervical Radiculopathy
Neck Pain with Radiating Pain

If you have a patient who presents with a clinical pattern similar to that of cervical radiculopathy, here are some things to consider!
o If you do not know the common clinical findings no problem! Click here
Anatomy

Special Tests
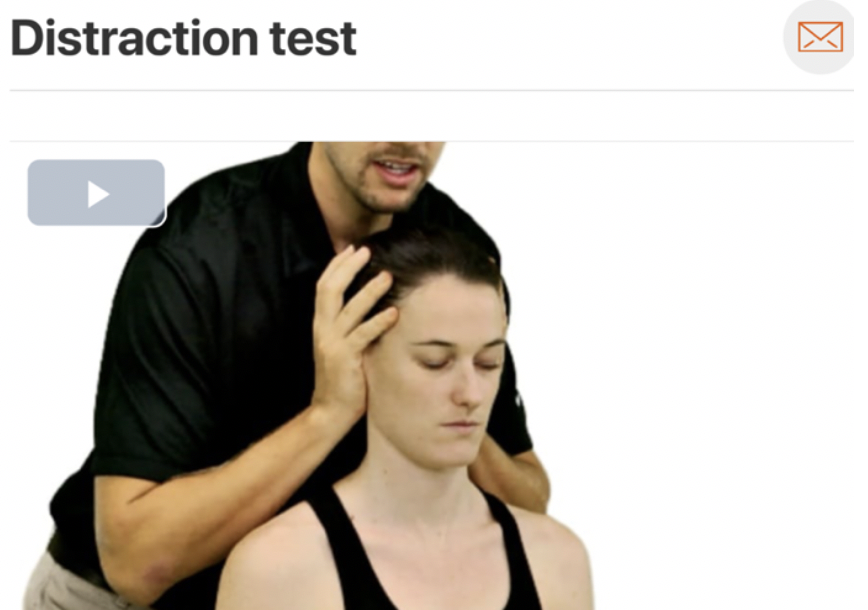

The above tests are part of the “Cervical Radiculopathy Cluster” designed to help the Physical Therapist better ascertain the likelihood of Cervical Radiculopathy as a diagnosis. Click the images to see how they are done!
Treatment
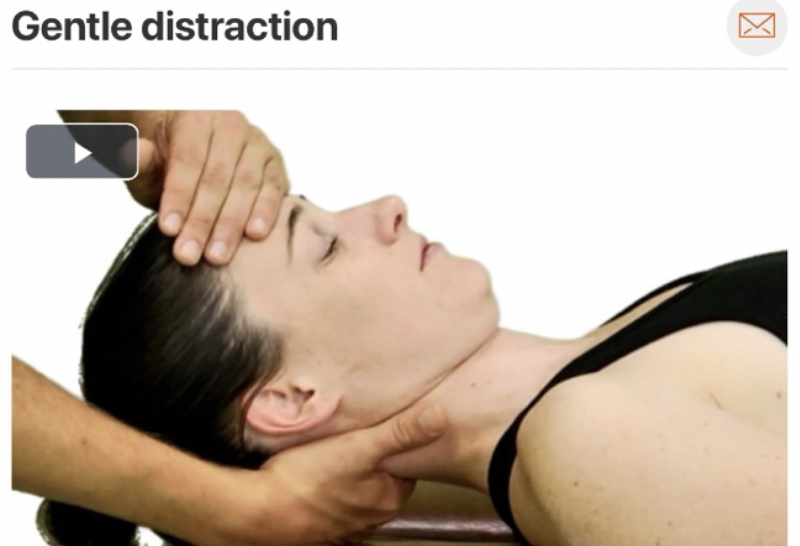
Gentle distraction of the cervical spine may be an appropriate initial intervention especially in patients with acute symptoms or those who are highly irritable.
Therapeutic Exercise


Therapeutic exercises chosen should always closely match treatment give in clinic; in this case self traction; however, do not forget to address posture!