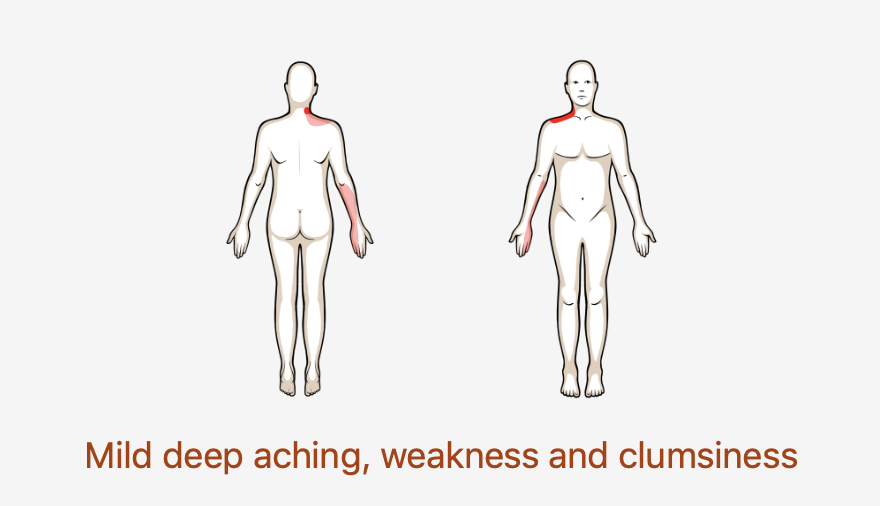
Shoulder Pain with Movement Coordination Impairments

Many labral tears are caused from shoulder dislocations. Anterior dislocations are most common and are often caused from a forceful collision, fall on an outstretched arm, or a sudden wrenching movement. The patient may present with apprehension at end ranges of motion.
If you do not know the common clinical findings no problem! Click here
Featured